Emergency departments are intense clinical environments, and correct documentation is critical not only for patient care but also for accurate billing and reimbursement. One of the most important areas influenced by documentation quality is E/M – Evaluation and Management – coding. E/M Coding Accuracy in ER depends on thorough, consistent, and compliant clinical notes. This is where ER medical scribes make a measurable difference by capturing each encounter in real time and ensuring that all necessary information is documented appropriately.
The Documentation Challenge and Its Impact on Coding
Emergency physicians face a heavy documentation burden. Research shows clinicians can spend nearly 40–50% of their workday on EHR and administrative tasks, leaving less time for direct patient care and precise documentation. When critical details are missing or incomplete, billers and coders struggle to assign the correct E/M level, which can result in undercoding, revenue loss, or compliance problems. Ensuring complete clinical narratives is fundamental to accurate coding and helps protect both patient safety and hospital reimbursement.
Real-time documentation by ER scribes supports providers by capturing histories, examinations, medical decision-making, and procedures as they occur. Instead of relying on memory or after-shift charting, scribes ensure that every relevant detail required to justify appropriate E/M levels is present and verifiable.
How Scribes Influence E/M Coding Accuracy
The Centers for Medicare & Medicaid Services (CMS) and other payers require documentation that supports the assigned E/M level, including components such as history, exam, and medical decision-making. In the rapid pace of emergency care, it is easy for clinicians to omit elements needed to support higher complexity levels. ER medical scribes help ensure that documentation reflects:
- Chief complaint and detailed history
- Objective findings and exam details
- Clinical decision-making complexity
- Procedures and results
By structuring notes according to payer guidelines and ensuring completeness, scribes reduce the risk of undercoding. Undercoding not only impacts reimbursement but also affects quality reporting, benchmarking, and performance metrics. Conversely, accurate documentation supports optimal E/M coding without resorting to upcoding, which carries legal and compliance risks.
Benefits of ER Medical Scribes for Coding and Billing
| Documentation Support | Coding & Billing Impact |
|---|---|
| Real-time clinical capture | Complete clinical picture supports correct E/M levels |
| Standardized templates | Consistency improves coder accuracy |
| Detailed exam notes | Better justification for higher complexity codes |
| Medical decision documentation | Accurately reflects clinical judgment |
| Procedure tracking | Ensures proper CPT code assignment |
Real-World Impact: Statistics and Evidence
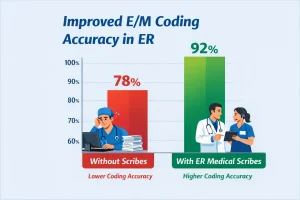
Multiple studies indicate that scribes help reduce missing or incomplete documentation, directly influencing coding accuracy. For example, research suggests that in emergency departments that use scribes, documentation completeness increases significantly, which correlates with improved coding outcomes and reduced downcoding due to missing elements.
In addition, departments that implement scribe support often report measurable improvements in workflow efficiency, provider satisfaction, and E/M capture rates. This not only protects revenue but also drives better operational performance and reduces the need for retrospective chart amendments — a common source of denials and auditing issues for coding teams.
Reducing Errors and Improving Data Integrity
Accurate clinical documentation is essential to patient safety, continuity of care, and billing integrity. Documentation gaps can lead to coding errors, claim denials, and compliance challenges. ER scribes help mitigate these issues by ensuring that provider notes are complete, clear, and reflective of actual clinical encounters.
In high-pressure emergency settings, scribes reduce omissions, inconsistencies, and documentation delays that can negatively impact coding and reimbursement.
Complete clinical documentation also supports downstream coding workflows. Coders rely on precise narratives to assign the correct ICD-10, CPT, and E/M codes. When scribes capture detailed clinical decision-making and exam findings, coders can confidently select higher, yet justified, E/M levels when appropriate, protecting revenue and reducing reliance on costly appeals.
Provider Experience and Productivity
One of the hidden benefits of improved documentation and coding accuracy is enhanced provider satisfaction. When physicians know that clinical notes are complete and supportive of correct coding, they spend less time reviewing and correcting charts after hours.
This contributes to reduced burnout, greater focus on clinical decision-making, and stronger engagement during patient encounters.
Improved note quality also supports clearer communication with patients, consultants, and other care team members, which in turn supports safer transitions of care and more accurate clinical handoffs.
Training and Best Practices for Scribe-Supported Coding
To maximize E/M coding accuracy, ER medical scribes should receive focused training on:
- Documentation standards for emergency care
- Key E/M coding criteria (history, exam, decision-making)
- Payer-specific guidelines and compliance nuances
- Best practices for structured notes and templates
Ongoing education and feedback loops between scribes, providers, and coding teams enhance documentation quality over time. When scribes understand what coders need to see, they can tailor notes that reduce ambiguity and support more accurate coding decisions.
Financial and Operational Benefits
Accurate E/M coding has clear financial implications. Undercoding leads to lost revenue, while overcoding exposes organizations to compliance scrutiny and potential penalties. By improving documentation completeness, ER medical scribes help optimize coding outcomes without sacrificing accuracy.
This supports a healthier revenue cycle, fewer claim denials, and better reimbursement capture.
In addition to protecting revenue, improved E/M Coding Accuracy in ER supports operational metrics such as chart completion time, throughput, and compliance readiness. Coders spend less time clarifying unclear documentation and more time processing accurate charts, which enhances overall departmental performance. For a deeper look into how scribes enhance emergency workflows, see how ER scribe solutions streamline documentation.
Conclusion: Elevating Documentation to Support Coding Excellence
In emergency medicine, accurate documentation is the foundation for correct E/M coding and financial integrity. ER medical scribes improve documentation completeness, reduce errors, and strengthen the connections between clinical care and proper billing. By capturing detailed clinical encounters in real time, scribes help ensure that E/M Coding Accuracy in ER reflects the true complexity of care delivered.
Investing in ER medical scribes supports not only better clinical notes but also a more efficient revenue cycle, reduced compliance risk, and improved provider experience. As emergency departments continue to face documentation challenges and coding complexity, scribes stand out as an essential part of high-performance care delivery.
Looking to improve E/M coding accuracy and protect your ER revenue cycle? Partner with a trusted scribe provider to enhance documentation quality, streamline workflows, and support compliance excellence. Request a customized quote today and discover how professional ER medical scribes can elevate both clinical performance and financial outcomes in your emergency department.